|
<< Click to Display Table of Contents >> Mental Status |
  
|
|
<< Click to Display Table of Contents >> Mental Status |
|
The Mental Status section of the Patient Medical Summaries reflect the patient's active cognitive status as entered in the Functional/Cognitive Status in the Health History application. "No Data Found" will display if no information is entered for the section or if No Impairment is documented within the application.
Select Patient Account > Health History > New > Referral/Transition of Care > Patient Medical Summaries > Patient Summary 2.1.4 > Mental Status
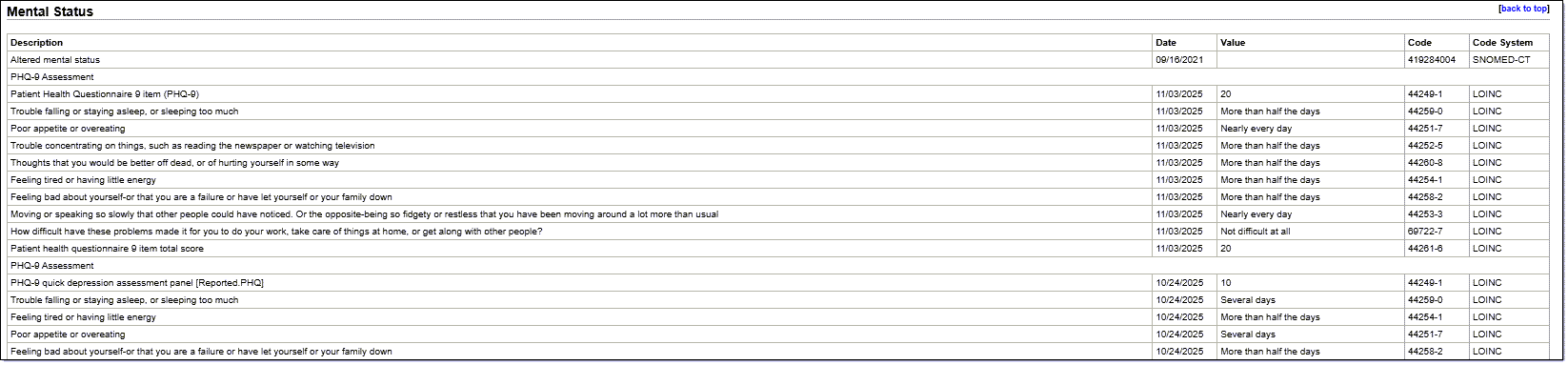
Mental Status
•Description: Displays the description of the impairment documented from the Health History Application-Functional/Cognitive Status section
•Date: Displays the Onset Date for the impairment documented
•Value: When the data is response to a questionnaire, e.g., PHQ-9 (LOINC 44249-1), PHQ-A (LOINC 44249-1), and GAD-7 General Anxiety Scale (LOINC 69737), the value of the selected answer is displayed here.
•Code: Displays the SNOMED Code associated with the impairment
•Code System: Displays the code system used for the identification of the mental impairment